

On July 1, 2016, the National Disability Insurance Scheme (NDIS) moved from a trial phase to a full national roll-out. In this series on Understanding the NDIS, we explore how the scheme works, why Australia needs it, and the issues to be addressed before eligible Australians, such as many Indigenous people with disability, can receive the benefits they are entitled to.
The National Disability Insurance Scheme (NDIS) is the only national scheme of its kind in the world. Its introduction has been likened to a generational shift with some saying the scheme’s impact will be similar to that of Medicare.
Choice and control are the fundamental principles of the NDIS, which represents a break from previous welfare approaches. The scheme aims to empower consumers with a disability to use funds given to them to purchase services that reflect their lifestyle and aspirations.
This aligns with the first principle of the United Nations Convention on the Rights of Persons with a Disability, to which Australia became a signatory in 2008. It’s based on neoliberalist ideology and models of consumerism where those who consume services also have choice, participation, rights and redress.
It’s hoped these changes will see the service sector reflect the interests of people with disabilities. This is the culmination of society’s evolution towards respecting, protecting and ensuring the rights of people with a disability.

Wellcome Images/Wikimedia Commons
The ‘deserving poor’
Prior to the 1600s in the United Kingdom, most people with a disability were cared for by their family. Public sentiment viewed those with disabilities as being sinners, possessed or moral degenerates (along with beggars criminals and prostitutes). They were often the focus of humour and humiliation.
Many with disabilities took refuge in monasteries from where they were sent to beg “cap in hand” – the source of the term handicap – for charity, and many did not live long.
The roots of the welfare model go back to the United Kingdom’s Elizabethan Poor Laws in 1601, which established parishes (jurisdictions reflecting land ownership by the gentry). These laws brought in the definition of the “impotent poor” – those unable to work and therefore to contribute to the local economy and parishes.
Under the welfare principle of “less eligibility”, housing and food provided to the impotent poor were so limited as to act as a disincentive to those believed to shirk work they could physically do. Nevertheless, the laws were the first recognition of the state’s responsibility to support the “deserving poor” – as opposed to the vagrants and layabouts.
The Poor Laws lasted more than 200 years, during which time people with disabilities remained impoverished and largely excluded from community. They lived hard and short lives in poorhouses funded through local taxation, relying on any other charity they received.
This model of charity and its associated philosophy influenced subsequent attempts to support people with disabilities in England, as well as Australia.
Large institutions known as asylums, designed to house people with mental illness and disabilities, were then built from the 1850s onwards evolving to reflect the growth of science and claims that medicine held a cure. History has condemned these asylums, which sometimes housed more than a thousand residents, as regimented and cruel.
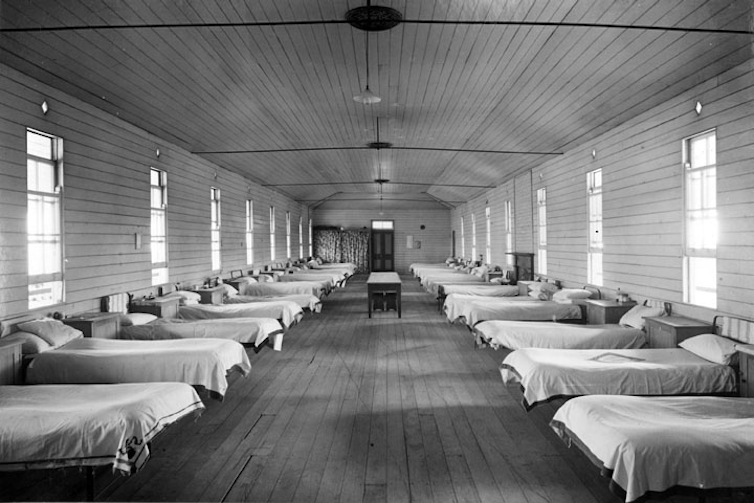
Agriculture And Stock Department, Publicity Branch/Wikimedia Commons
In these institutions, residents gave up decision-making, autonomy and identity to the system, which led to calls to release them from institutions into the community.
In the community but not ‘of it’
Resettlement back into the community started around the 1970s in Australia. Community care policies aimed to provide support, education, employment, housing and inclusion services.
Forty years after community care started, people with disabilities are living longer. Yet in 2009, a report based on consultation with people with disabilities found there was still little social inclusion, poor quality disability services and high unemployment.
Block funding and services assuming a one-size-fits-all approach were common under the welfare model. Funding went directly to a provider of goods and services, not the person buying the services. And the limited range of services couldn’t respond to the diverse needs of people with disabilities.
Then in 2011, the Productivity Commission found the support system gave people with disability little choice and no certainty of access to appropriate supports. It recommended that since most families and individuals could not prepare for the risk and financial impact of disability in their family, a scheme similar to Medicare based on insurance, should be implemented. So came the NDIS.
Under then Prime Minister Julia Gillard, a levy was introduced for all taxpayers, so anyone would benefit from the scheme if needed. Such insurance schemes are not new and have previously been used in places such as Victoria by the Traffic Accident Commission for those injured in road accidents.
Even though participants must be assessed as having a significant and enduring disability (a continuation of one aspect of the old welfare model), a progressive pillar of the NDIS is that block funding is replaced with individualised funding packages.
Issues with ‘choice for all’
If none of the NDIS elements are unique on their own, their combination is new and innovative. The NDIS seems a worthy investment which, on the face of it, achieves our common wish to treat all humans with dignity and as equal citizens.
But there are several issues still to be resolved. How to maximise choice remains a key problem – particularly for those unable to make these choices without support.
The majority of NDIS participants are electing to have their funds financially managed for them, or co-managed with agencies. Only 7% solely self-manage their funds. The National Disability Insurance Agency emphasises that people with disabilities can still make their own choices even where they do not manage their own finances, but this is yet to be seen.
Many of the other scheme’s benefits remain untested. The present arrangements raise questions about the effect on those who don’t qualify for funding packages – such as those with episodic or temporary illnesses and impairments requiring some level of support, but not sufficient to access NDIS funding. The Information, Linkage and Capacity building (ILC) framework has been designed to support these groups but clear evidence on coverage and outcomes from the trial sites is yet to emerge.
Finally, in a largely individualised system, the place of the collective voice of people with disabilities – the voice that helped the NDIS through parliament – is yet to feature. We need continual transformation and funding capable of maintaining a consistent dialogue for change between the NDIS as duty bearers and people with disabilities as rights holders.
You can read the accompanying piece on how the NDIS works and who is eligible for funding under the scheme here![]()
– Paul Ramcharan, Associate Professor, Centre for Applied Social Research, RMIT University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Feature Image Source: Pixabay





{kind=link}
{kind=link}
Leave A Comment